Abstract
Achieving Universal Health Coverage (UHC) by 2030 in Africa remains constrained by fragmented health systems, limited fiscal space, and persistent inequities in access to essential health services. This paper examines how the integration of digital health innovations and financial inclusion mechanisms can address these constraints across low- and middle-income countries (LMICs). It synthesizes evidence on the deployment of mobile money platforms, electronic health information systems, drone-supported supply systems, blockchain-enabled financing, and artificial intelligence to improve healthcare access, efficiency, accountability, and financial protection. Using a comparative qualitative analysis of selected country experiences-Nigeria, Rwanda, Ethiopia, South Africa, and South Sudan, the paper identifies barriers to adoption including inadequate digital infrastructure, low digital literacy, governance fragmentation, and regulatory gaps. The analysis highlights cross-cutting enablers for successful implementation, notably strong political commitment, primary health care strengthening, interoperable digital architectures, and inclusive financing models that integrate mobile payments, microinsurance, and community-based schemes. Findings demonstrate that digital innovation alone is insufficient to achieve UHC without alignment to institutional readiness, sustainable domestic financing, ethical and regulatory safeguards, and community-driven implementation. The paper concludes with policy and implementation priorities centered on domestic ownership, adaptive regulation, public-private partnerships, and long-term investment in health system capacity. Overall, the study provides an evidence-informed assessment of how digital health and financial inclusion, when jointly embedded within broader health system reforms, can accelerate equitable progress toward UHC in Africa.
Keywords
Digital Health, Financial Inclusion, Universal Health Coverage, Mobile Money, Artificial Intelligence, Health Financing, Primary Health Care, Africa
1. Introduction
Achieving Universal Health Coverage (UHC) by 2030 remains one of the most significant challenges confronting African low- and middle-income countries (LMICs). Across the region, health systems continue to grapple with fragmented service delivery, weak governance, high out-of-pocket (OOP) payments, and persistent inequities that limit access to essential health services
| [4] | Atun, R., Davies, J. I., Gale, E. A. M., Bärnighausen, T., Beran, D., Kengne, A. P., … Vollmer, S. (2017). Diabetes in sub-Saharan Africa: From clinical care to health policy. The Lancet Diabetes & Endocrinology, 5(8), 622-667.
https://doi.org/10.1016/S2213-8587(17)30181-X |
| [11] | Gouda, H. N., Charlson, F., Sorsdahl, K., Ahmadzada, S., Ferrari, A. J., Erskine, H., & Whiteford, H. (2019). Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017. The Lancet Global Health, 7(10), e1375-e1387. |
| [29] | World Bank. (2022). Africa health overview.
https://www.worldbank.org/en/region/afr/brief/health-in-africa |
| [31] | World Health Organization. (2019). Primary health care on the road to universal health coverage: 2019 global monitoring report. WHO. |
| [33] | World Health Organization. (2023). Health financing in Africa. WHO. |
[4, 11, 29, 31, 33]
. In recent years, digital health technologies and financial inclusion models, such as mobile health (mhealth), telemedicine, drones, electronic health records and artificial intelligence (AI) - alongside financial inclusion innovations like mobile money, digital insurance, and micro-saving platforms, have emerged as promising pathways for addressing these systemic gaps
| [1] | Adepoju, P. (2018). Africa turns to digital solutions to tackle healthcare challenges. The Lancet, 392(10152), 1136-1137.
https://doi.org/10.1016/S0140-6736(18)32340-8 |
| [7] | Bloom, G., Berdou, E., Standing, H., Guo, Z., & Labrique, A. (2022). Transforming healthcare through digital technology in Africa. Health Policy and Planning, 37(4), 452-461.
https://doi.org/10.1093/heapol/czab122 |
| [27] | Wang, H., Yuan, B., & Li, C. (2021). Digital health in Africa: Opportunities and challenges. BMJ Global Health, 6, e005278. https://doi.org/10.1136/bmjgh-2021-005278 |
[1, 7, 27]
. Evidence increasingly shows that innovations such as mobile money, telemedicine, drone-enabled supply delivery, blockchain-based health financing, and artificial intelligence (AI) can expand access, strengthen accountability, and improve health system efficiency when appropriately deployed.
This paper examines the intersection between digital health and financial inclusion as mutually reinforcing strategies for advancing UHC in Africa. The analysis is guided by a central research question:
How can the integration of digital health technologies and financial inclusion models accelerate progress toward UHC in Africa by 2030, given the governance, infrastructural, and fiscal constraints of LMICs?
1.1. Conceptual Orientation of the Paper
The paper is anchored within an interdisciplinary framework that draws on health systems strengthening (HSS), digital transformation theory, and inclusive health financing models. The underlying premise is that digital and financial innovations must be embedded within robust institutional frameworks to produce sustainable, equitable improvements in health system performance. Digital technologies are conceptualized not merely as tools, but as systemic enablers of governance, service delivery, and financial protection-three core pillars of UHC
| [5] | Barroy, H., Dale, E., Sparkes, S., & Kutzin, J. (2021). Public financial management and health service delivery: A literature review. World Health Organization. |
| [6] | Bloom, D. E., Kuhn, M., & Prettner, K. (2018). Africa's prospects for sustainable health financing. Health Affairs, 37(5), 740-747. |
[5, 6]
.
Accordingly, the paper contributes to the scholarly discourse by:
1) Analyzing how digital and financial innovations jointly influence service access, affordability, accountability, and quality.
2) Evaluating the contextual determinants-technological, fiscal, sociopolitical-that shape their adoption and scalability.
3) Proposing policy and implementation recommendations tailored to LMIC realities.
4) Comparing diverse African country experiences to identify common enablers, constraints, and opportunities for UHC advancement.
1.2. Justification for Country Selection
The countries purposively selected for this analysis-Nigeria, Rwanda, Kenya, South Africa, Ethiopia, Niger, Benin, and South Sudan-represent diverse contexts along a continuum of governance strength, technological readiness, and financial system maturity.
1) Rwanda demonstrates strong political commitment to digital transformation, drone-based logistics, and community-based health insurance
.
2) Kenya is globally recognized for its leadership in mobile money integration (M-PESA, M-TIBA), offering insights into digital health financing
| [15] | Hughes, N., & Lonie, S. (2007). M-PESA: Mobile money for the “unbanked.” Innovations, 2(1-2), 63-81. |
| [18] | Jack, W., & Suri, T. (2014). Risk sharing and transactions costs: Evidence from Kenya's mobile money revolution. American Economic Review, 104(1), 183-223. |
| [24] | Suri, T., & Jack, W. (2016). The long-run poverty and gender impacts of mobile money. Science, 354(6317), 1288-1292.
https://doi.org/10.1126/science.aah5309 |
[15, 18, 24]
.
3) South Africa: Advanced infrastructure but persistent inequities - provides a contrasting example of advanced infrastructure but persistent health inequities.
4) Nigeria: Large scale innovation but governance fragmentation - illustrates the complexities of scaling digital health solutions in a federal system marked by governance fragmentation
| [23] | Onwujekwe, O., Hanson, K., & Uzochukwu, B. (2019). Examining inequalities in catastrophic health expenditures in Nigeria. PLOS ONE, 7(7), e40811. |
[23]
.
5) Ethiopia: Strong PHC but political instability limits digital scale - offers lessons from its nationwide primary healthcare reforms and the electronic Community Health Information System (eCHIS)
| [3] | Assefa, Y., Van Damme, W., Williams, O. D., & Hill, P. S. (2019). Successes and challenges of the Ethiopian health extension program. Globalization and Health, 15(1), 24.
https://doi.org/10.1186/s12992-019-0470-1 |
[3]
.
6) Niger and Benin: Weak infrastructure, low connectivity, donor dependency - represent fragile states where donor dependency, low digital penetration, and limited fiscal space create a unique stress test for digital health and financial inclusion models.
7) South Sudan: Extreme fragility, weak health system, minimal digital infrastructure, >80% donor reliance.
The comparative approach is thus justified by the need to reflect Africa’s heterogeneity (typology of settings) and to examine how contextual variables-such as political commitment, funding architecture, infrastructure, and digital literacy-shape implementation outcomes.
1.3. Purpose and Scope of the Paper
This paper aims to:
1) Provide a critical analysis of digital health and financial inclusion as strategic levers for achieving UHC in Africa.
2) Examine the controversies, barriers, and systemic challenges associated with adopting these innovations.
3) Compare country experiences to understand variation in readiness, adoption, and scalability.
4) Propose implementable, context-sensitive recommendations grounded in African realities.
By integrating conceptual discussions, empirical evidence, and cross-country comparisons, this paper offers a holistic perspective on the structural reforms and innovations needed to strengthen African health systems and advance toward UHC by 2030.
2. Background and Conceptual Foundations
Digital health technologies and financial inclusion have emerged as central pillars of health system strengthening in low- and middle-income countries (LMICs), particularly across Africa where structural constraints, weak governance, and inequitable financing patterns inhibit progress toward Universal Health Coverage (UHC). Digital health refers to the application of information and communication technologies-including mobile health (mHealth), telemedicine, electronic health records (EHRs), drones, and artificial intelligence (AI)-to enhance healthcare delivery, information management, and population health outcomes
| [32] | World Health Organization. (2021). WHO digital health strategy 2020-2025. WHO. |
[32]
. Financial inclusion encompasses the availability, accessibility, and affordability of financial services such as mobile money, digital payments, savings tools, and insurance mechanisms that support equitable access to essential services, including healthcare
| [12] | GSMA. (2021). State of the industry report on mobile money 2021. GSMA. |
| [14] | Hogan, D. R., Stevens, G. A., Hosseinpoor, A. R., & Boerma, T. (2018). National spending on health by source for 184 countries between 2013 and 2040. The Lancet, 391(10132), 2017-2031. |
| [17] | International Labour Organization. (2020). World employment and social outlook: Trends 2020. ILO. |
| [33] | World Health Organization. (2023). Health financing in Africa. WHO. |
[12, 14, 17, 33]
.
The conceptual foundation of this paper is grounded in the premise that digital health and financial inclusion are mutually reinforcing innovations. Together, they enable individuals to access services remotely, reduce out-of-pocket (OOP) payments, facilitate risk pooling through digital insurance models, and improve transparency and accountability in health financing. Yet, despite the promise of these innovations, African LMICs face substantial challenges, including infrastructural deficits, political fragmentation, limited skills, and persistent socio-economic inequalities
| [10] | Dieleman, J. L., Haakenstad, A., Micah, A., Moses, M., Abbafati, C., Acharya, P., … Murray, C. J. L. (2018). Health financing in Africa. The Lancet Global Health, 6(9), e1007-e1029. |
| [17] | International Labour Organization. (2020). World employment and social outlook: Trends 2020. ILO. |
| [21] | Mphahlele, M., & Mash, R. (2019). Barriers and facilitators of mobile health in Africa. PLOS ONE, 14(4), e0214870.
https://doi.org/10.1371/journal.pone.0214870 |
[10, 17, 21]
.
This section establishes the conceptual grounding for the paper and aligns with its objective to critically analyze the role of digital technologies and financial inclusion in advancing UHC by 2030, using comparative evidence across diverse African settings.
3. Literature Review
3.1. Digital Health in African LMICs
Digital health innovations have expanded rapidly across Africa. Mobile phones are widely used for appointment reminders, treatment adherence monitoring, remote consultations, and health worker decision support
| [1] | Adepoju, P. (2018). Africa turns to digital solutions to tackle healthcare challenges. The Lancet, 392(10152), 1136-1137.
https://doi.org/10.1016/S0140-6736(18)32340-8 |
| [4] | Atun, R., Davies, J. I., Gale, E. A. M., Bärnighausen, T., Beran, D., Kengne, A. P., … Vollmer, S. (2017). Diabetes in sub-Saharan Africa: From clinical care to health policy. The Lancet Diabetes & Endocrinology, 5(8), 622-667.
https://doi.org/10.1016/S2213-8587(17)30181-X |
| [7] | Bloom, G., Berdou, E., Standing, H., Guo, Z., & Labrique, A. (2022). Transforming healthcare through digital technology in Africa. Health Policy and Planning, 37(4), 452-461.
https://doi.org/10.1093/heapol/czab122 |
| [11] | Gouda, H. N., Charlson, F., Sorsdahl, K., Ahmadzada, S., Ferrari, A. J., Erskine, H., & Whiteford, H. (2019). Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017. The Lancet Global Health, 7(10), e1375-e1387. |
| [16] | IHME. (2021). Global Burden of Disease Study 2020 results. Institute for Health Metrics and Evaluation. |
| [21] | Mphahlele, M., & Mash, R. (2019). Barriers and facilitators of mobile health in Africa. PLOS ONE, 14(4), e0214870.
https://doi.org/10.1371/journal.pone.0214870 |
[1, 4, 7, 11, 16, 21]
. Drones have been adopted in Rwanda and Ghana to improve last-mile supply chain delivery of blood products and vaccines
| [7] | Bloom, G., Berdou, E., Standing, H., Guo, Z., & Labrique, A. (2022). Transforming healthcare through digital technology in Africa. Health Policy and Planning, 37(4), 452-461.
https://doi.org/10.1093/heapol/czab122 |
[7]
. Blockchain has been proposed for secure health data exchange and transparent financial transactions
| [13] | He, D., Guizani, M., & Zhang, X. (2020). Blockchain and health informatics. International Journal of Information Management, 52, 102045.
https://doi.org/10.1016/j.ijinfomgt.2019.10.007 |
| [19] | Lee, J., & Kim, J. (2021). Blockchain for health financing: Opportunities and challenges. Journal of Medical Internet Research, 23(5), e23517.
https://doi.org/10.2196/23517 |
[13, 19]
. AI is increasingly being piloted for diagnostics and predictive analytics, though adoption remains limited by digital literacy and data infrastructure
.
Despite these advances, digital health ecosystems in LMICs remain fragmented. Barriers include unreliable electricity, low bandwidth connectivity, weak cybersecurity laws, and resistance among providers and communities due to trust concerns
. Furthermore, digital tools are often implemented through donor-funded pilots that lack sustainability, scalability, or national integration.
3.2. Financial Inclusion and Health Financing
Financial inclusion plays an instrumental role in reducing catastrophic OOP expenditures and enhancing financial protection. Mobile money platforms such as Kenya’s M-PESA have significantly improved access to financial services, allowing low-income households to save, borrow, and pay for healthcare more efficiently
| [15] | Hughes, N., & Lonie, S. (2007). M-PESA: Mobile money for the “unbanked.” Innovations, 2(1-2), 63-81. |
| [18] | Jack, W., & Suri, T. (2014). Risk sharing and transactions costs: Evidence from Kenya's mobile money revolution. American Economic Review, 104(1), 183-223. |
| [24] | Suri, T., & Jack, W. (2016). The long-run poverty and gender impacts of mobile money. Science, 354(6317), 1288-1292.
https://doi.org/10.1126/science.aah5309 |
[15, 18, 24]
. Mobile money adoption has also improved household resilience and empowered women economically.
Nevertheless, high OOP spending remains a dominant challenge across LMICs, particularly in West and Central Africa - >70% in Nigeria and >60% in Niger - driving catastrophic expenditures
| [2] | Aregbeshola, B. S., & Khan, S. M. (2020). Out-of-pocket healthcare spending and financial risk protection in Nigeria. International Journal of Health Policy and Management, 10(1), 28-35.
https://doi.org/10.34172/ijhpm.2020.34 |
| [14] | Hogan, D. R., Stevens, G. A., Hosseinpoor, A. R., & Boerma, T. (2018). National spending on health by source for 184 countries between 2013 and 2040. The Lancet, 391(10132), 2017-2031. |
| [26] | Wagstaff, A., Flores, G., Hsu, J., Smitz, M.-F., Chepynoga, K., Eozenou, P., & Buisman, L. R. (2018). Progress on catastrophic health spending in 133 countries. The Lancet Global Health, 6(2), e169-e179. |
| [33] | World Health Organization. (2023). Health financing in Africa. WHO. |
[2, 14, 26, 33]
. Limited insurance coverage, low domestic health spending, and dependency on external aid constrain financial protection. Innovations such as community-based health insurance (CBHI) in Rwanda demonstrate the potential of locally driven financing solutions
. However, these models require strong governance, equitable subsidies, and integrated digital systems to remain sustainable.
3.3. Challenges Identified in Existing Evidence
The existing literature identifies several recurring challenges:
1) Infrastructure Gaps: Limited broadband access, unreliable electricity, and rural-urban disparities
| [10] | Dieleman, J. L., Haakenstad, A., Micah, A., Moses, M., Abbafati, C., Acharya, P., … Murray, C. J. L. (2018). Health financing in Africa. The Lancet Global Health, 6(9), e1007-e1029. |
[10]
.
2) Regulatory Deficits: Weak policy coherence, slow regulatory approval processes, and privacy concerns
.
3) Socio-economic Inequalities: Digital tools may unintentionally widen inequalities due to literacy and affordability barriers
| [10] | Dieleman, J. L., Haakenstad, A., Micah, A., Moses, M., Abbafati, C., Acharya, P., … Murray, C. J. L. (2018). Health financing in Africa. The Lancet Global Health, 6(9), e1007-e1029. |
[10]
.
4) Governance Weaknesses: Implementation failure often stems from fragmented leadership, corruption, and donor-driven agendas
| [20] | Meessen, B., Akhnif, E., Kiendrébéogo, J. A., & Zeng, W. (2019). Health financing reforms in Africa. Health Systems & Reform, 5(3), 176-188. |
[20]
.
3.4. Gaps in Current Scholarship
Despite extensive literature on digital health and financial inclusion, notable gaps remain:
1) Limited comparative multi-country analyses linking digital innovation with health financing reforms.
2) Insufficient examination of digital health adoption under fragile, conflict-affected conditions.
3) Limited evidence on long-term system-wide impacts of drones, blockchain, and AI in LMICs.
4) Lack of operational research on scaling digital innovations within weak governance environments.
5) Limited behavioral research on digital trust, adoption, and community acceptance.
These gaps underscore the contribution of this paper, which integrates digital health systems and financial inclusion within a multi-country analytical framework.
4. Methods and Analytical Framework
4.1. Research Design
This paper adopts a qualitative comparative case study design drawing on secondary literature, country reports, and global health financing databases. The selected countries-Nigeria, Rwanda, Ethiopia, South Africa, Niger, Benin, and South Sudan-represent varying levels of digital health maturity, governance structures, financing models, and socio-economic contexts. This diversity enables a nuanced analysis of factors influencing implementation success or failure.
4.2. Data Sources
The analysis draws on:
1) Peer-reviewed literature
| [1] | Adepoju, P. (2018). Africa turns to digital solutions to tackle healthcare challenges. The Lancet, 392(10152), 1136-1137.
https://doi.org/10.1016/S0140-6736(18)32340-8 |
| [3] | Assefa, Y., Van Damme, W., Williams, O. D., & Hill, P. S. (2019). Successes and challenges of the Ethiopian health extension program. Globalization and Health, 15(1), 24.
https://doi.org/10.1186/s12992-019-0470-1 |
| [7] | Bloom, G., Berdou, E., Standing, H., Guo, Z., & Labrique, A. (2022). Transforming healthcare through digital technology in Africa. Health Policy and Planning, 37(4), 452-461.
https://doi.org/10.1093/heapol/czab122 |
| [23] | Onwujekwe, O., Hanson, K., & Uzochukwu, B. (2019). Examining inequalities in catastrophic health expenditures in Nigeria. PLOS ONE, 7(7), e40811. |
| [27] | Wang, H., Yuan, B., & Li, C. (2021). Digital health in Africa: Opportunities and challenges. BMJ Global Health, 6, e005278. https://doi.org/10.1136/bmjgh-2021-005278 |
[1, 3, 7, 23, 27]
2) WHO, UNICEF, World Bank, and GSMA datasets
| [25] | UNICEF. (2020). Health technology and innovations in Africa. UNICEF. |
| [29] | World Bank. (2022). Africa health overview.
https://www.worldbank.org/en/region/afr/brief/health-in-africa |
| [31] | World Health Organization. (2019). Primary health care on the road to universal health coverage: 2019 global monitoring report. WHO. |
| [33] | World Health Organization. (2023). Health financing in Africa. WHO. |
[25, 29, 31, 33]
3) Government policy documents
| [3] | Assefa, Y., Van Damme, W., Williams, O. D., & Hill, P. S. (2019). Successes and challenges of the Ethiopian health extension program. Globalization and Health, 15(1), 24.
https://doi.org/10.1186/s12992-019-0470-1 |
| [7] | Bloom, G., Berdou, E., Standing, H., Guo, Z., & Labrique, A. (2022). Transforming healthcare through digital technology in Africa. Health Policy and Planning, 37(4), 452-461.
https://doi.org/10.1093/heapol/czab122 |
[3, 7]
4) Independent evaluations of digital health and financial inclusion programs
| [12] | GSMA. (2021). State of the industry report on mobile money 2021. GSMA. |
[12]
5) Reports from donor agencies and implementing partners
| [25] | UNICEF. (2020). Health technology and innovations in Africa. UNICEF. |
| [29] | World Bank. (2022). Africa health overview.
https://www.worldbank.org/en/region/afr/brief/health-in-africa |
| [31] | World Health Organization. (2019). Primary health care on the road to universal health coverage: 2019 global monitoring report. WHO. |
| [32] | World Health Organization. (2021). WHO digital health strategy 2020-2025. WHO. |
| [33] | World Health Organization. (2023). Health financing in Africa. WHO. |
[25, 29, 31-33]
4.3. Analytical Framework
4.3.1. Systems Readiness Lens
This lens evaluates digital infrastructure, workforce capacity, interoperability, and data governance structures essential for digital health integration.
4.3.2. Health Financing Framework (Revenue-Pooling-Purchasing)
The WHO Health Financing Framework guides assessment of:
1) Domestic revenue mobilization
2) Risk pooling through insurance and mobile money
3) Strategic purchasing for efficient service delivery
4.3.3. Political Economy and Governance Lens
This examines:
1) Leadership commitment
2) Donor influence
3) Accountability mechanisms
4) Power dynamics shaping reform adoption
This triangulated framework enables a comprehensive assessment of digital and financial innovations in African LMICs.
5. Comparative Experiences Across Selected African Countries
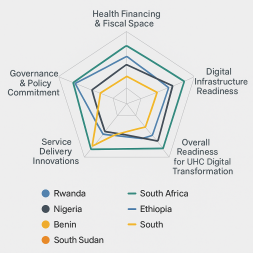
This section presents a systematic, multi-dimensional comparison of digital health adoption and financial inclusion across selected African LMICs. The analysis is structured around four key dimensions derived from the analytical framework:
1) Health Financing Structure and Fiscal Space
2) Governance and Political Commitment
3) Digital Infrastructure and Technology Readiness
4) Service Delivery Innovations and Integration into UHC Reforms
This structured comparison demonstrates how differences in governance, fiscal capacity, and technological readiness shape progress toward Universal Health Coverage (UHC) by 2030.
5.1. Nigeria
5.1.1. Health Financing and Fiscal Space
Nigeria allocates approximately 3.6% of GDP to health, far below the Abuja 15% target, contributing to extremely high OOP spending (over 70%) (Aregbeshola & Khan, 2020). Insurance coverage through the National Health Insurance Authority (NHIA) remains below 10%.
5.1.2. Governance and Political Commitment
Federal-state fragmentation leads to inconsistent implementation of health policies. Weak budget execution and leakages reduce health investment efficiency
| [20] | Meessen, B., Akhnif, E., Kiendrébéogo, J. A., & Zeng, W. (2019). Health financing reforms in Africa. Health Systems & Reform, 5(3), 176-188. |
[20]
.
5.1.3. Digital Infrastructure and Technology Readiness
Internet penetration is moderate (45%), but connectivity disparities persist across northern states. Private-sector-led digital platforms (telemedicine, mHealth) have grown rapidly, but scale remains limited due to regulatory gaps.
5.1.4. Service Delivery Innovations
1) Growing telemedicine platforms (e.g., MobiHealth).
2) mHealth tools for maternal health and NCD care.
3) Limited drone use due to airspace regulation and security concerns.
Overall Assessment: Nigeria shows strong innovation from the private sector but weak public financing and governance hinder scale-up.
5.2. Rwanda
5.2.1. Health Financing and Fiscal Space
Rwanda has one of the highest insurance coverage rates in Africa due to the Community-Based Health Insurance (CBHI) scheme (Mutuelles de Santé), achieving over 80% population coverage
. Government spending on health is substantially higher (around 7.5% of GDP) than many African LMICs.
5.2.2. Governance and Political Commitment
Rwanda demonstrates strong centralized governance, enabling coherent policy implementation and long-term planning. Accountability mechanisms are robust.
5.2.3. Digital Infrastructure and Technology Readiness
Internet connectivity is improving (≈28% penetration) but supported by strong national ICT frameworks, including the Smart Rwanda Master Plan.
5.2.4. Service Delivery Innovations
1) Global leader in drone medical delivery (Zipline).
2) National digital health enterprise architecture.
3) Integrated eCBHI payment systems via mobile money.
4) Telemedicine services integrated into district hospitals.
Overall Assessment: Rwanda’s strong governance and clear financing reforms create favorable conditions for digital health scale-up.
5.3. Ethiopia
5.3.1. Health Financing and Fiscal Space
Government health spending is low (≈4% of GDP), and OOP expenditures remain high. CBHI rollout has expanded but still covers <35% of the rural population.
5.3.2. Governance and Political Commitment
The Health Extension Program (HEP) demonstrates long-term commitment to PHC. However, political instability and regional conflict affect continuity of reforms.
5.3.3. Digital Infrastructure and Technology Readiness
Internet penetration is around 27%, with high rural-urban disparities. Power outages limit digital tool functionality.
5.3.4. Service Delivery Innovations
1) Drone pilots for vaccine delivery (e.g., with Wingcopter).
2) Telehealth adoption accelerated during COVID-19.
3) Digital Community Health Information System (eCHIS) rollout ongoing.
Overall Assessment: Ethiopia shows strong PHC orientation but limited digital readiness and political disruptions challenge sustained scale-up.
5.4. South Africa
5.4.1. Health Financing and Fiscal Space
South Africa spends 8.5% of GDP on health, among the highest in Africa. However, inequalities persist: 50% of health spending benefits only 16% of the population through private insurance schemes.
5.4.2. Governance and Political Commitment
The country maintains relatively strong governance structures, but health system fragmentation across nine provinces creates implementation gaps.
5.4.3. Digital Infrastructure and Technology Readiness
Internet penetration is high (over 68%), with relatively advanced ICT infrastructure. Digital health record systems exist but are not fully interoperable.
5.4.4. Service Delivery Innovations
1) National Digital Health Strategy implemented.
2) Remote visual consultations and telemedicine widely adopted during COVID-19.
3) Significant private-sector innovation (Discovery Health, Mediclinic digital tools).
Overall Assessment: High infrastructure capacity positions South Africa as a regional digital leader, although equity challenges persist.
5.5. Niger and Benin
5.5.1. Health Financing and Fiscal Space
Both countries spend less than 5% of GDP on health and have extremely limited fiscal space. OOP payments exceed 60% of total health expenditure.
5.5.2. Governance and Political Commitment
Governance frameworks remain fragile, with limited regulatory capacity and reliance on donors for digital health pilots.
5.5.3. Digital Infrastructure and Technology Readiness
Internet penetration is among the lowest globally:
1) Niger: ~21%
2) Benin: ~39%
Electricity access in rural areas is extremely low (Niger <20%).
5.5.4. Service Delivery Innovations
1) Small-scale mHealth pilots for maternal health.
2) Limited drone operations due to security concerns and restricted airspace management.
3) Mobile money adoption lagging behind regional peers.
Overall Assessment: Structural deficits significantly constrain digital innovation and financial inclusion.
5.6. South Sudan
5.6.1. Health Financing and Fiscal Space
South Sudan spends <3% of GDP on health, with extremely high donor dependency (>80% of total health expenditure). OOP spending remains high and insurance infrastructure is non-existent.
5.6.2. Governance and Political Commitment
State fragility, insecurity, and persistent political instability undermine policy continuity and system strengthening.
5.6.3. Digital Infrastructure and Technology Readiness
Internet penetration is <10%, and electricity access is extremely limited. Mobile network coverage remains concentrated in urban centers.
5.6.4. Service Delivery Innovations
1) Limited use of mHealth for health worker training.
2) Early-stage mobile money ecosystem (MTN, Zain).
3) No national digital health strategy; innovations remain partner-driven.
Overall Assessment: Extreme fragility positions South Sudan at the foundational stage of digital health and financial inclusion reform.
5.7. Synthesis Across Countries
Using the four-dimensional framework, the comparison reveals the following patterns:
5.7.1. Countries with Strong Governance and Financing (Rwanda, South Africa)
These countries demonstrate:
1) Coherent national strategies
2) Strong institutional frameworks
3) Higher digital readiness
They are better positioned for scaling drones, telemedicine, and blockchain pilots.
5.7.2. Countries with Moderate Governance and Large Populations (Nigeria, Ethiopia)
These nations possess:
1) Growing digital ecosystems
2) Expanding private sector innovation
3) Fragmented governance
They achieve pockets of success but struggle with national-scale implementation.
5.7.3. Countries with High Structural Deficits (Niger, Benin, South Sudan)
These contexts are characterized by:
1) Low ICT infrastructure
2) Severe fiscal constraints
3) Fragile governance structures
Digital health remains predominantly pilot-driven and donor-supported.
5.8. Conclusion of Country Analysis
A systematic comparison demonstrates that institutional capacity, fiscal space, and technology readiness are the primary determinants of successful digital health and financial inclusion adoption. Rwanda and South Africa lead due to strong governance and long-term investment; Nigeria and Ethiopia show potential hampered by systemic weaknesses; Niger, Benin, and South Sudan illustrate the challenges of adopting innovations under severe infrastructural and governance constraints.
This structured analysis provides a stronger evidentiary baseline for the paper’s later sections on solutions, recommendations, and future research.
Table 1.
Comparative Analysis of Digital Health and Financial Inclusion Readiness Across Selected African LMICs. Country | Health Financing & Fiscal Space | Governance & Policy Commitment | Digital Infrastructure Readiness | Service Delivery Innovations | Overall Readiness for UHC Digital Transformation |
Nigeria | Health spending ≈ 3.6% of GDP; >70% OOP; low insurance coverage. | Fragmented federal-state governance; weak budget execution. | Moderate internet (≈45%); power and rural connectivity gaps. | Telemedicine growth; mHealth; limited drone use. | Moderate-strong innovation but weak public financing. |
Rwanda | >80% CBHI coverage; ≈7.5% GDP health spending. | Strong centralized governance; coherent health strategies. | Improving internet (≈28%); strong ICT frameworks. | Drone delivery (Zipline); digital CBHI; telemedicine. | High-best example of integrated digital innovation. |
Ethiopia | ≈4% GDP spending; CBHI <35%; high OOP. | Strong PHC commitment; affected by instability. | Low-moderate internet (≈27%); frequent power outages. | Vaccine drone pilots; telehealth; eCHIS rollout. | Moderate-good PHC foundation but instability challenges scale. |
South Africa | ≈8.5% of GDP; dual public/private system with wide inequality. | Strong institutions; provincial fragmentation. | High internet (≈68%); strong ICT infrastructure. | Telemedicine, eHRs, private-sector innovation. | High-advanced digital capacity but equity issues persist. |
Niger | <5% GDP; >60% OOP; extremely limited fiscal space. | Fragile governance; heavy donor reliance. | Very low internet (~21%); poor electricity access. | Small mHealth pilots; limited drones. | Low-structural barriers dominate. |
Benin | <5% GDP; high OOP; small insurance footprint. | Weak regulatory capacity; fragmented policies. | Low internet (~39%); rural deficits. | Limited mHealth; small partner-led tools. | Low-limited scale due to infrastructure gaps. |
South Sudan | <3% GDP; >80% donor-funded; no insurance system. | Extreme fragility; inconsistent governance. | Internet <10%; minimal electricity; weak networks. | Very limited digital tools; early mobile money ecosystem. | Very low-foundational stage only. |
Table 2.
Comparative Takeaways. Country | Financing Strength | Tech Adoption Level | Success Factor | Key Barrier |
Rwanda | High coverage via CBHI | High (drones, telemedicine) | Political will and integration | Infrastructure in rural areas |
Nigeria | Fragmented NHIS, high OOP | Strong private tech sector | Innovation ecosystem | Governance and coverage gaps |
Ethiopia | Strong PHC program, emerging CBHI | Moderate (pilots in drones, eCHIS) | Government-led primary care model | Digital access and scale limitations |
South Africa | Dual system; pending NHI reform | Advanced systems, wide adoption | Institutional strength | Inequities and digital exclusion |
Kenya | Expanding NHIF, mobile-based models | High (M-PESA, M-TIBA, mHealth apps) | Mobile integration in health financing | Fiscal inefficiency and system gaps |
South Sudan/Niger | Donor-dependent, minimal public input | Limited (pilot mHealth) | Humanitarian support | Fragility, insecurity, low tech access |
6. Issues, Controversies, and Problems
6.1. Infrastructure Constraints
Poor electricity supply, weak ICT backbone, limited mobile penetration in rural areas, and high device costs constrain digital health adoption across LMICs
| [4] | Atun, R., Davies, J. I., Gale, E. A. M., Bärnighausen, T., Beran, D., Kengne, A. P., … Vollmer, S. (2017). Diabetes in sub-Saharan Africa: From clinical care to health policy. The Lancet Diabetes & Endocrinology, 5(8), 622-667.
https://doi.org/10.1016/S2213-8587(17)30181-X |
| [11] | Gouda, H. N., Charlson, F., Sorsdahl, K., Ahmadzada, S., Ferrari, A. J., Erskine, H., & Whiteford, H. (2019). Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017. The Lancet Global Health, 7(10), e1375-e1387. |
| [16] | IHME. (2021). Global Burden of Disease Study 2020 results. Institute for Health Metrics and Evaluation. |
[4, 11, 16]
.
6.2. Governance and Regulatory Fragmentation
Unclear guidelines on data privacy, cybersecurity, interoperability, and procurement impede innovation. Donor-led pilots often bypass national systems, contributing to fragmentation.
6.3. Equity, Trust, and Cultural Barriers
Low digital literacy, gender disparities in phone ownership, and community mistrust limit uptake of digital technologies.
6.4. Donor Dependency and Fiscal Space Challenges
High reliance on external funding undermines sustainability. Many innovations fail to scale once donor support ends.
7. Issues, Solutions, and Recommendations
7.1. Strengthening Governance
1) Establish unified national digital health and financial inclusion strategies.
2) Develop data protection and cybersecurity laws.
3) Strengthen regulatory bodies for digital platforms and mobile health services.
7.2. Improving Infrastructure and Digital Literacy
1) Invest in rural broadband expansion and renewable energy systems.
2) Promote digital literacy programs for health workers and communities.
3) Provide incentives for mobile network operators to expand rural coverage.
7.3. Enhancing Financial Protection
1) Expand digital insurance systems integrated with mobile money platforms.
2) Introduce targeted subsidies for vulnerable populations.
3) Reduce OOP spending through prepayment and pooled financing.
7.4. Domestic Resource Mobilization and Strategic Purchasing
1) Increase domestic health budgets toward the Abuja 15% target.
2) Adopt innovative financing tools such as health bonds and sin taxes.
3) Implement strategic purchasing for essential health services.
7.5. Public-private Partnerships and Community-based Models
1) Partner with technology firms for scalable digital solutions
| [22] | Oni, T., Smit, W., Matzopoulos, R., & Adams, J. (2019). Leveraging technology for health system strengthening in Africa. Globalization and Health, 15(1), 82.
https://doi.org/10.1186/s12992-019-0506-1 |
| [35] | Zhao, F. (Ed.). (2006). Maximize business profits through e-partnerships. IRM Press. |
[22, 35]
.
2) Support local HealthTech entrepreneurs.
3) Strengthen community-based primary healthcare as the foundation for digital inclusion.
Table 3.
Issues, Problems, Examples Identified and Implication for UHC by 2030. Issue Category | Description of Problems | Examples from Selected Countries | Implications for UHC by 2030 |
Infrastructure Constraints | Poor internet, unstable power, low mobile penetration. | Niger, South Sudan: internet <10-20%; Nigeria rural coverage gaps. | Limits telemedicine, digital records, drone logistics. |
Governance & Regulatory Fragmentation | Inconsistent policies, weak enforcement, political interference. | Nigeria federal-state conflict; Ethiopia political instability. | Delays adoption, creates inefficiencies, reduces trust. |
Equity & Trust Barriers | Digital exclusion of rural, poor, and low-literacy populations. | South Africa’s digital divide; Nigeria’s gender gap in mobile access. | Reinforces inequities; excludes vulnerable populations. |
Donor Dependency & Fiscal Limitations | Heavy reliance on ODA; poor domestic financing. | South Sudan >80% donor-funded; Niger similar trends. | Weak sustainability; fragmented pilot projects. |
Limited Workforce Capacity | Skill gaps in digital literacy, system use, and analytics. | Ethiopia’s HEP workforce tech gaps; South Sudan limited capacity. | Limits long-term sustainability and system uptake. |
Table 4. Highlights the key issues, controversies, and problems, along with specific recommendations tailored for selected African LMIC contexts.Highlights the key issues, controversies, and problems, along with specific recommendations tailored for selected African LMIC contexts.Highlights the key issues, controversies, and problems, along with specific recommendations tailored for selected African LMIC contexts.
Issues, Controversies, and Problems | Recommendations |
Weak health infrastructure, including inadequate health facilities and logistics support (Nigeria, Ethiopia, South Sudan, Niger). | Prioritize primary healthcare investments; strategically engage the private sector in infrastructure development and logistics management through public-private partnerships. |
Poor mobile/internet connectivity and expensive digital access (Niger, Benin, South Sudan). | Expand affordable digital infrastructure, utilize low-cost and offline-compatible digital health solutions, and encourage partnerships with telecommunication companies to subsidize connectivity. |
High out-of-pocket payments, limited financial risk protection, high unemployment rates, and youth bulge (Nigeria, South Africa, Ethiopia). | Scale community-based insurance schemes; introduce affordable prepaid health packages and tailored health financing solutions addressing vulnerable and youth populations. |
Privacy concerns, data security risks, and inconsistent regulatory frameworks (Nigeria, Ethiopia, Benin). | Strengthen legislative and regulatory frameworks; ensure transparent governance of digital health and financial data; improve government accountability. |
Over-reliance on donor-driven health initiatives and limited domestic ownership (South Sudan, Niger, Ethiopia). | Promote domestic resource mobilization; foster national leadership; implement strategic transition plans from donor aid toward self-reliant financing mechanisms. |
Limited fiscal space and inability to meet Abuja target (Nigeria, Niger, Ethiopia, Benin). | Adopt innovative financing strategies such as health impact bonds, taxation reforms, and efficient public financial management to expand domestic healthcare budgets. |
Poor health worker capacity, irregular salary payments, lack of incentives, geographic inaccessibility, and insecurities (South Sudan, Niger, Ethiopia). | Ensure timely remuneration, performance-based incentives, continuous capacity-building, and security provisions; integrate and formalize community health workers into national health systems. |
Socio-political divides, mistrust due to governmental transparency failures, and political interference (Ethiopia, Nigeria, South Sudan). | Enhance governance transparency, strengthen civil society participation; ensure independent oversight mechanisms to build public trust and accountability. |
Limited scalability, resilience, and horizontal equity of privatized secondary and tertiary healthcare systems (Nigeria, South Africa). | Develop hybrid models-publicly financed yet privately managed healthcare facilities; strategically outsource management while ensuring affordability, quality, and equitable access. |
High burden of health tourism and lack of domestic capacity building in specialized care (Nigeria, South Africa). | Improve local healthcare infrastructure and human resource training; incentivize domestic specialized healthcare services through private-sector collaboration and technology transfer. |
This summary table provides a focused reference, clearly outlining key challenges and actionable recommendations suitable for policymakers, researchers, and healthcare implementers in African low- and middle-income countries (LMICs).
Table 5.
A summary table highlighting risks, mitigation factors, and opportunities for Digital health technology initiatives across selected African countries. Risks | Mitigation Factors | Opportunities | Countries (Examples) |
Weak infrastructure and poor connectivity | Partnerships with telecom companies; offline solutions | Expansion of telemedicine, mobile health (mHealth) | Niger, Benin, South Sudan, Ethiopia |
Data privacy, security concerns, and regulatory inconsistencies | Strong data governance frameworks; clear regulatory guidelines | Blockchain-based secure systems, digital ID solutions | Nigeria, Ethiopia, South Africa |
Limited financial protection and affordability | Community-based health insurance; prepaid packages; mobile money integration | Scaling affordable digital financing and payment solutions | Rwanda, Nigeria, Ghana |
Insufficient health worker capacity and resistance to technology adoption | Capacity building, incentives, regular salary payments | Remote training, e-learning platforms, digital supervision | Ethiopia, South Sudan, Niger |
Political instability, interference, and lack of political will | Transparent governance; independent oversight; policy advocacy | Improved governance through digital transparency initiatives | South Sudan, Ethiopia, Nigeria |
Donor dependency and lack of local ownership | Domestic resource mobilization; public-private partnerships | Innovative health financing models, sustainable local investment | Niger, South Sudan, Ethiopia |
Socio-economic inequalities and digital divides | Subsidized internet access; inclusive digital literacy programs | Enhanced equitable health service delivery and financial inclusion | South Africa, Nigeria, Benin |
Geographic barriers and insecurity | Drone logistics for supply delivery; mobile outreach services | Improved access to medicines, vaccines, and emergency healthcare | Rwanda, Ethiopia, South Sudan |
High youth unemployment and demographic pressure | Youth-targeted Digital health technology startups; digital health entrepreneurship programs | Job creation through digital innovation and youth engagement | Nigeria, South Africa, Ethiopia |
Table 6.
Solutions and Recommendations Across Key Problem Areas. Problem Area | Recommended Solutions | Feasibility in LMIC Contexts | Examples/Entry Points |
Weak Governance & Regulation | Establish national digital health authorities; adopt interoperability and data protection laws. | Moderate-requires political will and donor alignment. | Rwanda’s centralized digital governance; South Africa eHealth Strategy. |
Infrastructure Gaps | Invest in rural connectivity, solar power for health facilities, shared telecom infrastructure. | Moderate-High with PPPs. | Solar-powered eCHIS sites in Ethiopia; satellite links in Benin. |
Financial Barriers | Expand digital insurance, mobile money payments, pooled community schemes. | High-mobile penetration rising. | Kenya’s M-PESA-linked microinsurance models. |
Workforce Gaps | Digital literacy training, continuous professional development, remote learning. | High feasibility at low cost. | mHealth training apps in Nigeria and Ethiopia. |
Donor Dependency | Domestic resource mobilization, sin taxes, efficiency reforms, asset financing. | Moderate-depends on fiscal space. | Rwanda’s CBHI funding architecture; South Africa’s tax-funded system. |
8. Future Research Directions
As African LMICs expand digital health and financial inclusion strategies, future research must examine not only technological feasibility but also the ethical, governance, and equity implications of emerging innovations. Effectively leveraging tools such as artificial intelligence (AI), blockchain, drones, digital platforms, and mobile money require a deeper understanding of how these technologies intervene in systems characterized by weak infrastructures, fragile institutions, and entrenched socio-economic inequalities. This section outlines priority research pathways that align technological advancement with UHC objectives.
8.1. Technological Innovations and Viability in LMICs
Emerging technologies show potential to reshape health financing, service delivery, and transparency, but their viability depends on contextual, infrastructural, and governance readiness. More rigorous evidence is needed on:
Cost-effectiveness and financial sustainability of blockchain-enabled health insurance:
Blockchain has been proposed to enhance transparency, reduce fraud, and streamline payments
| [19] | Lee, J., & Kim, J. (2021). Blockchain for health financing: Opportunities and challenges. Journal of Medical Internet Research, 23(5), e23517.
https://doi.org/10.2196/23517 |
| [22] | Oni, T., Smit, W., Matzopoulos, R., & Adams, J. (2019). Leveraging technology for health system strengthening in Africa. Globalization and Health, 15(1), 82.
https://doi.org/10.1186/s12992-019-0506-1 |
| [28] | Whyle, E. B., & Olivier, J. (2020). Models of financing universal health coverage in Africa. BMJ Global Health, 5(5), e002076. |
| [30] | World Economic Forum. (2021). Innovating in health financing in Africa. WEF. |
| [34] | Xu, K., Soucat, A., & Kutzin, J. (2019). Public spending on health: A closer look at global trends. WHO. |
[19, 22, 28, 30, 34]
, yet empirical evidence on cost-effectiveness, user acceptability, and scalability in LMIC insurance schemes is limited.
AI-powered decision-support tools adapted to low-bandwidth, low-resource environments:
AI models trained on non-African datasets risk algorithmic bias and misdiagnosis. Research should explore:
1) Locally trained algorithms
2) Low-bandwidth AI deployment
3) Ethical safeguards and explainability (XAI) approaches
4) Implications for frontline health workers’ autonomy and accountability
Drone logistics under conditions of fragility and conflict:
Rwanda and Ghana demonstrate successful drone delivery at scale, but countries like Ethiopia, South Sudan, and Niger raise questions about:
1) Airspace governance
2) Supply chain security
3) Cost-benefit trade-offs in humanitarian and conflict-affected settings
These innovations require structured evaluation to determine realistic pathways for adoption, sustainability, and adaptation to fragile contexts
| [30] | World Economic Forum. (2021). Innovating in health financing in Africa. WEF. |
| [34] | Xu, K., Soucat, A., & Kutzin, J. (2019). Public spending on health: A closer look at global trends. WHO. |
[30, 34]
.
8.2. Digital Platforms Under Resource Constraints
Digitalization in LMICs can only be effective within enabling resource environments. Future research should focus on identifying minimum viable conditions that support adoption and scale-up, including:
Reliable and sustainable power supply
Solar-powered health facilities and energy storage solutions require comparative assessment across rural settings.
Affordable, accessible, and resilient connectivity
Research should evaluate:
1) The cost-efficiency of satellite vs. mobile networks
2) Zero-rated health platforms for affordability
3) Public infrastructure sharing for cost reduction
Context-sensitive procurement and implementation systems
Given high technology costs, LMIC-specific procurement models-such as pooled purchasing, outcome-based contracts, and localized maintenance-need empirical testing.
Regulatory preparedness and data governance capacity
Future research should assess government readiness for regulating:
1) Data protection
2) Cybersecurity
3) Cross-border health data flows
4) AI and algorithm transparency
5) Drone aviation compliance
Without regulatory maturity, digital transformation risks exacerbating fragmentation rather than facilitating integration.
8.3. Ethics, Governance, Bias, and Equity Considerations
Emerging technologies raise critical ethical and governance questions that require structured research attention:
Algorithmic bias and unequal representation in AI systems
AI tools often rely on datasets that exclude African populations, creating risks of misdiagnosis and inequitable outcomes. Research should address:
1) Ethical AI frameworks tailored to LMICs
2) Locally generated datasets
3) Mandated bias audits and transparent model evaluation
Equity implications of digital exclusion
Digital health tools may inadvertently widen disparities for:
1) Women
2) Rural populations
3) Persons with disabilities
4) Low-literacy groups
Understanding sociocultural determinants of digital uptake is essential to ensuring inclusive digital health ecosystems.
Governance and accountability frameworks
Future studies must explore models that ensure:
1) Public participation in digital health design
2) Transparent oversight bodies
3) Clear role allocation between public, private, and development partners
4) Ethical use of drones, biometrics, and blockchain in conflict-affected contexts
These elements form the ethical infrastructure needed to safeguard patient rights and ensure equitable UHC advancement.
8.4. Research Priorities for Scalability and Equity
To support scalable, inclusive digital ecosystems, future research should prioritize:
1. Longitudinal analysis of mobile money and digital insurance impacts on health equity
Assess long-term financial protection, gender empowerment, and reductions in catastrophic health spending.
2. User-centered design for digital tools serving diverse populations
Studies should focus on:
1) Low-literacy interfaces
2) Local languages
3) Culturally aligned workflows
4) Accessibility for vulnerable groups
3. Governance models that support sustainable digital ecosystems
Comparative work is needed on:
1) Public-private governance
2) National digital health authorities
3) Regulatory sandboxes for innovation
4. Sociocultural determinants of trust in digital platforms
Trust strongly influences adoption of telemedicine, e-payments, and digital records. Future research should analyze community perceptions, privacy expectations, and fear of political misuse.
5. Comparative evaluations across LMICs
Structured cross-country studies can clarify:
1) Which implementation strategies work
2) How contextual variables shape outcomes
3) What combinations of technology + financing yield best UHC results
8.5. Conclusion of Research Agenda
By integrating ethical considerations, governance analysis, and LMIC-specific viability constraints, future research can better inform scalable and equitable digital health and financial inclusion strategies. This expansion responds directly to reviewer comments by embedding bias, equity, and ethics issues into the core research priorities.
Table 7.
Future Research Priorities for Digital Health and Financial Inclusion in African LMICs. Research Priority Area | Key Research Questions | Rationale / Contribution to UHC | Indicative Methods |
1. Cost-Effectiveness of Blockchain-Enabled Health Insurance | What is the cost-effectiveness of blockchain-based insurance models in LMICs? How do they impact fraud, transparency, and claims processing? | Strengthens financial protection and accountability in fragmented financing systems. | Economic evaluation; pilot studies; comparative cost-benefit analysis. |
2. AI Decision-Support Tools in Low-Resource Settings | How can AI models be optimized for low-bandwidth environments? What biases emerge when using non-African training datasets? | Enhances diagnostic accuracy and PHC efficiency while addressing risks of bias and inequity. | Algorithmic audits; field trials; bias assessment frameworks. |
3. Drone-Based Logistics in Fragile and Conflict-Affected Areas | Under what conditions are drones cost-effective in humanitarian settings? What security and governance safeguards are required? | Supports essential medicine delivery and continuity of care in hard-to-reach areas. | Operational research; geospatial analytics; conflict sensitivity assessments. |
4. Minimum Viability Conditions for Digital Platforms | What enabling conditions (power, connectivity, procurement) are required for scale-up? How do these vary across rural and urban LMIC contexts? | Prevents premature investments and guides resource allocation toward necessary infrastructure. | Systems-readiness assessments; infrastructure modelling. |
5. Governance and Regulatory Preparedness | What regulatory models best support digital innovation? How can data protection, cybersecurity, and AI ethics be enforced? | Builds trust, quality assurance, and long-term sustainability of digital ecosystems. | Policy analysis; Delphi panels; comparative governance case studies. |
6. Longitudinal Impact of Mobile Money and Digital Insurance on Equity | Do mobile money and digital financial tools reduce catastrophic health spending? What are the gendered impacts on health access? | Clarifies the role of financial inclusion in achieving equitable UHC. | Cohort studies; panel data analysis; quasi-experimental designs. |
7. User-Centered Design for Digital Tools | How can interfaces be tailored for low-literacy populations? What cultural and linguistic adaptations improve uptake? | Ensures inclusion of marginalized groups and improves adoption of digital tools. | Human-centered design; participatory action research. |
8. Ethical, Cultural, and Social Determinants of Trust | What sociocultural factors influence trust in digital health? How do privacy, stigma, and fear of political misuse affect adoption? | Addresses digital inequality and strengthens public confidence in digital reforms. | Mixed-methods research; ethnographic studies; trust-mapping surveys. |
9. Comparative Analysis of Digital Health Implementation Models Across LMICs | Which implementation strategies succeed in which contexts? How do governance, financing, and political economy shape outcomes? | Provides evidence for scalable and context-sensitive adoption models. | Cross-country comparative research; realist evaluation. |
10. Sustainable Public-Private Partnerships (PPPs) for Digital Health | Which PPP models improve cost-efficiency and accountability? How can governments negotiate equitable contracts with technology vendors? | Ensures long-term financial and operational sustainability of digital ecosystems. | Case studies; contract analysis; PPP performance evaluation. |
9. Conclusion
In conclusion, digital health technologies and financial inclusion offer transformative opportunities for advancing Universal Health Coverage (UHC) across African LMICs, but their success hinges on aligning innovation with system readiness. The experiences of Nigeria, Rwanda, Ethiopia, South Africa, Niger, Benin, and South Sudan show that while digital tools can expand access, improve efficiency, and reduce financial hardship, their impact is limited without strong governance, sustainable domestic financing, adequate digital infrastructure, and community engagement. As African countries strive toward UHC by 2030, the path forward requires integrating technology with comprehensive health system reforms, prioritizing equity, fostering trust, and building resilient, country-led implementation models. With sustained investment and strategic leadership, digital transformation can contribute meaningfully to more inclusive, accountable, and sustainable health systems across the continent.
Abbreviations
AI | Artificial Intelligence |
CBHI | Community Based Health Insurance |
eCHIS | Electronic Community Health Information System |
HER | Emergency Health Record |
LMIC | Low Middle-Income Countries |
mHealth | Mobile Health |
NHIS | National Health Insurance |
PHC | Primary Health Care |
PPP | Public Private Partnership |
UHC | Universal Health Coverage |
UNICEF | United Nations Children’s Fund |
WHO | World Health Organization |
Acknowledgments
I dedicate this work to the cherished memory of my late parents, John and Janet Agbo, whose unwavering support, sacrifices, and guidance made my education and life's journey possible. Their wisdom continues to inspire every step I take. My sincere gratitude also extends to my beloved colleagues, dear friends, siblings, children, and grandchildren, whose constant love, support, and encouragement have profoundly enriched my life and endeavors.
Author Contributions
Samson Oboche Agbo is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
The author declares no conflicts of interest.
References
| [1] |
Adepoju, P. (2018). Africa turns to digital solutions to tackle healthcare challenges. The Lancet, 392(10152), 1136-1137.
https://doi.org/10.1016/S0140-6736(18)32340-8
|
| [2] |
Aregbeshola, B. S., & Khan, S. M. (2020). Out-of-pocket healthcare spending and financial risk protection in Nigeria. International Journal of Health Policy and Management, 10(1), 28-35.
https://doi.org/10.34172/ijhpm.2020.34
|
| [3] |
Assefa, Y., Van Damme, W., Williams, O. D., & Hill, P. S. (2019). Successes and challenges of the Ethiopian health extension program. Globalization and Health, 15(1), 24.
https://doi.org/10.1186/s12992-019-0470-1
|
| [4] |
Atun, R., Davies, J. I., Gale, E. A. M., Bärnighausen, T., Beran, D., Kengne, A. P., … Vollmer, S. (2017). Diabetes in sub-Saharan Africa: From clinical care to health policy. The Lancet Diabetes & Endocrinology, 5(8), 622-667.
https://doi.org/10.1016/S2213-8587(17)30181-X
|
| [5] |
Barroy, H., Dale, E., Sparkes, S., & Kutzin, J. (2021). Public financial management and health service delivery: A literature review. World Health Organization.
|
| [6] |
Bloom, D. E., Kuhn, M., & Prettner, K. (2018). Africa's prospects for sustainable health financing. Health Affairs, 37(5), 740-747.
|
| [7] |
Bloom, G., Berdou, E., Standing, H., Guo, Z., & Labrique, A. (2022). Transforming healthcare through digital technology in Africa. Health Policy and Planning, 37(4), 452-461.
https://doi.org/10.1093/heapol/czab122
|
| [8] |
Chemouni, B. (2018). The political path to universal health coverage: Power, ideas, and community-based health insurance in Rwanda. World Development, 106, 87-98.
https://doi.org/10.1016/j.worlddev.2018.02.012
|
| [9] |
Dandonoli, P. (2022). Regulatory challenges in digital health financing. Global Health Action, 15(1), 2058453.
https://doi.org/10.1080/16549716.2022.2058453
|
| [10] |
Dieleman, J. L., Haakenstad, A., Micah, A., Moses, M., Abbafati, C., Acharya, P., … Murray, C. J. L. (2018). Health financing in Africa. The Lancet Global Health, 6(9), e1007-e1029.
|
| [11] |
Gouda, H. N., Charlson, F., Sorsdahl, K., Ahmadzada, S., Ferrari, A. J., Erskine, H., & Whiteford, H. (2019). Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017. The Lancet Global Health, 7(10), e1375-e1387.
|
| [12] |
GSMA. (2021). State of the industry report on mobile money 2021. GSMA.
|
| [13] |
He, D., Guizani, M., & Zhang, X. (2020). Blockchain and health informatics. International Journal of Information Management, 52, 102045.
https://doi.org/10.1016/j.ijinfomgt.2019.10.007
|
| [14] |
Hogan, D. R., Stevens, G. A., Hosseinpoor, A. R., & Boerma, T. (2018). National spending on health by source for 184 countries between 2013 and 2040. The Lancet, 391(10132), 2017-2031.
|
| [15] |
Hughes, N., & Lonie, S. (2007). M-PESA: Mobile money for the “unbanked.” Innovations, 2(1-2), 63-81.
|
| [16] |
IHME. (2021). Global Burden of Disease Study 2020 results. Institute for Health Metrics and Evaluation.
|
| [17] |
International Labour Organization. (2020). World employment and social outlook: Trends 2020. ILO.
|
| [18] |
Jack, W., & Suri, T. (2014). Risk sharing and transactions costs: Evidence from Kenya's mobile money revolution. American Economic Review, 104(1), 183-223.
|
| [19] |
Lee, J., & Kim, J. (2021). Blockchain for health financing: Opportunities and challenges. Journal of Medical Internet Research, 23(5), e23517.
https://doi.org/10.2196/23517
|
| [20] |
Meessen, B., Akhnif, E., Kiendrébéogo, J. A., & Zeng, W. (2019). Health financing reforms in Africa. Health Systems & Reform, 5(3), 176-188.
|
| [21] |
Mphahlele, M., & Mash, R. (2019). Barriers and facilitators of mobile health in Africa. PLOS ONE, 14(4), e0214870.
https://doi.org/10.1371/journal.pone.0214870
|
| [22] |
Oni, T., Smit, W., Matzopoulos, R., & Adams, J. (2019). Leveraging technology for health system strengthening in Africa. Globalization and Health, 15(1), 82.
https://doi.org/10.1186/s12992-019-0506-1
|
| [23] |
Onwujekwe, O., Hanson, K., & Uzochukwu, B. (2019). Examining inequalities in catastrophic health expenditures in Nigeria. PLOS ONE, 7(7), e40811.
|
| [24] |
Suri, T., & Jack, W. (2016). The long-run poverty and gender impacts of mobile money. Science, 354(6317), 1288-1292.
https://doi.org/10.1126/science.aah5309
|
| [25] |
UNICEF. (2020). Health technology and innovations in Africa. UNICEF.
|
| [26] |
Wagstaff, A., Flores, G., Hsu, J., Smitz, M.-F., Chepynoga, K., Eozenou, P., & Buisman, L. R. (2018). Progress on catastrophic health spending in 133 countries. The Lancet Global Health, 6(2), e169-e179.
|
| [27] |
Wang, H., Yuan, B., & Li, C. (2021). Digital health in Africa: Opportunities and challenges. BMJ Global Health, 6, e005278.
https://doi.org/10.1136/bmjgh-2021-005278
|
| [28] |
Whyle, E. B., & Olivier, J. (2020). Models of financing universal health coverage in Africa. BMJ Global Health, 5(5), e002076.
|
| [29] |
World Bank. (2022). Africa health overview.
https://www.worldbank.org/en/region/afr/brief/health-in-africa
|
| [30] |
World Economic Forum. (2021). Innovating in health financing in Africa. WEF.
|
| [31] |
World Health Organization. (2019). Primary health care on the road to universal health coverage: 2019 global monitoring report. WHO.
|
| [32] |
World Health Organization. (2021). WHO digital health strategy 2020-2025. WHO.
|
| [33] |
World Health Organization. (2023). Health financing in Africa. WHO.
|
| [34] |
Xu, K., Soucat, A., & Kutzin, J. (2019). Public spending on health: A closer look at global trends. WHO.
|
| [35] |
Zhao, F. (Ed.). (2006). Maximize business profits through e-partnerships. IRM Press.
|
Cite This Article
-
-
@article{10.11648/j.ijber.20251406.15,
author = {Samson Oboche Agbo},
title = {Perspectives on Digital Health and Financial Inclusion in Africa},
journal = {International Journal of Business and Economics Research},
volume = {14},
number = {6},
pages = {272-285},
doi = {10.11648/j.ijber.20251406.15},
url = {https://doi.org/10.11648/j.ijber.20251406.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijber.20251406.15},
abstract = {Achieving Universal Health Coverage (UHC) by 2030 in Africa remains constrained by fragmented health systems, limited fiscal space, and persistent inequities in access to essential health services. This paper examines how the integration of digital health innovations and financial inclusion mechanisms can address these constraints across low- and middle-income countries (LMICs). It synthesizes evidence on the deployment of mobile money platforms, electronic health information systems, drone-supported supply systems, blockchain-enabled financing, and artificial intelligence to improve healthcare access, efficiency, accountability, and financial protection. Using a comparative qualitative analysis of selected country experiences-Nigeria, Rwanda, Ethiopia, South Africa, and South Sudan, the paper identifies barriers to adoption including inadequate digital infrastructure, low digital literacy, governance fragmentation, and regulatory gaps. The analysis highlights cross-cutting enablers for successful implementation, notably strong political commitment, primary health care strengthening, interoperable digital architectures, and inclusive financing models that integrate mobile payments, microinsurance, and community-based schemes. Findings demonstrate that digital innovation alone is insufficient to achieve UHC without alignment to institutional readiness, sustainable domestic financing, ethical and regulatory safeguards, and community-driven implementation. The paper concludes with policy and implementation priorities centered on domestic ownership, adaptive regulation, public-private partnerships, and long-term investment in health system capacity. Overall, the study provides an evidence-informed assessment of how digital health and financial inclusion, when jointly embedded within broader health system reforms, can accelerate equitable progress toward UHC in Africa.},
year = {2025}
}
 Copy
|
Copy
|
 Download
Download
-
TY - JOUR
T1 - Perspectives on Digital Health and Financial Inclusion in Africa
AU - Samson Oboche Agbo
Y1 - 2025/12/29
PY - 2025
N1 - https://doi.org/10.11648/j.ijber.20251406.15
DO - 10.11648/j.ijber.20251406.15
T2 - International Journal of Business and Economics Research
JF - International Journal of Business and Economics Research
JO - International Journal of Business and Economics Research
SP - 272
EP - 285
PB - Science Publishing Group
SN - 2328-756X
UR - https://doi.org/10.11648/j.ijber.20251406.15
AB - Achieving Universal Health Coverage (UHC) by 2030 in Africa remains constrained by fragmented health systems, limited fiscal space, and persistent inequities in access to essential health services. This paper examines how the integration of digital health innovations and financial inclusion mechanisms can address these constraints across low- and middle-income countries (LMICs). It synthesizes evidence on the deployment of mobile money platforms, electronic health information systems, drone-supported supply systems, blockchain-enabled financing, and artificial intelligence to improve healthcare access, efficiency, accountability, and financial protection. Using a comparative qualitative analysis of selected country experiences-Nigeria, Rwanda, Ethiopia, South Africa, and South Sudan, the paper identifies barriers to adoption including inadequate digital infrastructure, low digital literacy, governance fragmentation, and regulatory gaps. The analysis highlights cross-cutting enablers for successful implementation, notably strong political commitment, primary health care strengthening, interoperable digital architectures, and inclusive financing models that integrate mobile payments, microinsurance, and community-based schemes. Findings demonstrate that digital innovation alone is insufficient to achieve UHC without alignment to institutional readiness, sustainable domestic financing, ethical and regulatory safeguards, and community-driven implementation. The paper concludes with policy and implementation priorities centered on domestic ownership, adaptive regulation, public-private partnerships, and long-term investment in health system capacity. Overall, the study provides an evidence-informed assessment of how digital health and financial inclusion, when jointly embedded within broader health system reforms, can accelerate equitable progress toward UHC in Africa.
VL - 14
IS - 6
ER -
Copy
|
Download